Risk of Type 1 Diabetes
If no diabetes in the family:- 0.1% , otherwise
If identical twin with Type 1 Diabetes:- 25-50%
If either parent has diabetes: (multiply the risk by 2 if parent was diagnosed with Type 1 Diabetes before age 11)
If father has Type 1 Diabetes:- 6%
If mother was younger than 25 at propositus's birth:- 4%
If mother was 25 or older at propositus's birth:- 1%
Ninety (90) % of Type 1 cases are
positive for a non-aspartic acid amino acid residue at
position HLA B57,
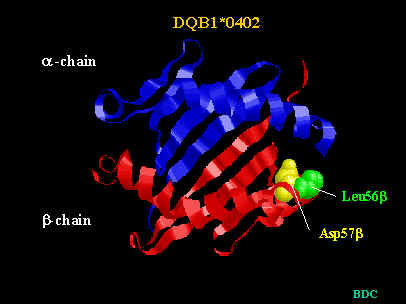
or VQbeta macrophage receptors, or Islet Cell Antibodies (anti-Glutamic
Acid Decarboxylase 64kd, anti-tyrosine phosphatase (Rabin
Ag512/IA-1), anti-insulin)